

10
Average IPC at-home drainage procedures per month4

0
ACES at-home drainage procedures per month3
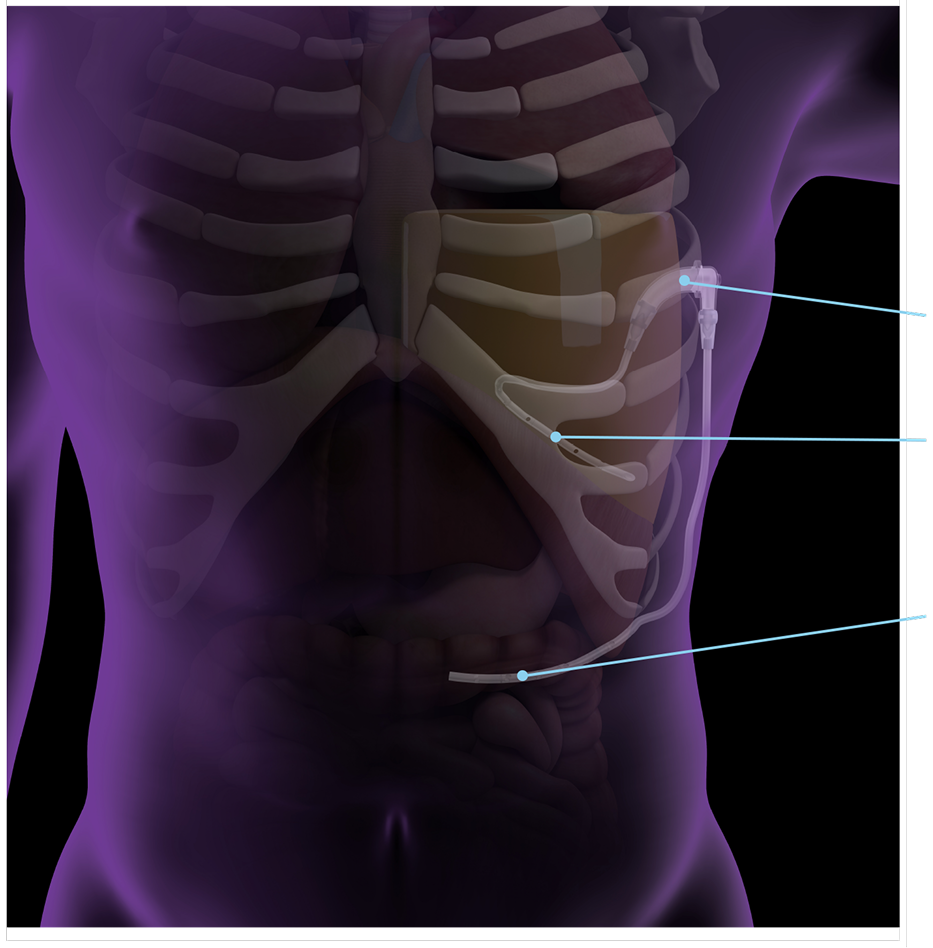

Pleural entry
Peritoneal entry

“Providing our patients with a solution that improves their quality of life and lessens the burden of maintaining an implanted medical device for their chronic medical condition has the potential to really change the way we manage pleural disease.”
—Dr. Jason Akulian, MD, Chapel Hill, NC

